
Of course we are being facetious when we use the word “scam.”
But it nevertheless reflects the opinion of a major portion of the US population that have, shall we say, doubts about the need, the efficacy, or the safety of the coronavirus vaccines that are (hopefully) rolling out in the coming weeks.
It is simply amazing to read the comments on social media from the anti-vax community.
From the microchips to the genetic alterations caused by “chemicals” in the vaccines, there is an endless stream of anti-vaccine nonsense out there.
The nonsense seems to fall into a few distinct camps:
Insufficient Testing – Time
For eons the pharmaceutical industry has lamented the lengthy clinical trial requirements imposed by governments.
But now, facing a global emergency, companies have responded in record time. This seems contradictory to some who cannot (ironically) believe that a drug can be developed so quickly.
Surely shortcuts were taken!
The reality, of course, is that the industry had been able to move unusually quickly, for several critical reasons:
- The SARS-CoV-2 genome was published in January. Making this information public and accessible accelerated the movement towards mRNA.
- The core technologies to make these vaccines were already in place and in development for other indications.
- The disease is highly prevalent in the US and EU countries, making rapid large-scale trial recruitment by CROs possible.
- Regulatory agencies are willing to accelerate their own processes (especially during a US election year) in order to sign off on the relevant stages of product development.
History will look back at this as a lesson in speed and coordination, and not a process based on shortcuts.
Insufficient Testing – Scale
Others are latching on to the idea that the trials were fast because they were too small and poorly powered.
Yet the facts do not support this.
The most recent Pfizer and Moderna trials alone recruited over 70,000 subjects combined.
To put that into perspective, the labelled trials for Shingrix had <30,000 subjects. These are Framingham-like numbers that will only increase once these products are approved.
Both ideas (Scale and Testing) reflect a general lack of understanding of how clinical trials work. Perhaps we should say that they reflect our industry’s inability to explain and communicate how the clinical trial process works without sounding whiny about it.
The general population does not understand that a clinical trial for one disease may take less time and be smaller than another.
As an industry, it is time to move away from our simplistic message of “trials are expensive and costly and risky, which is why drugs are expensive.”
Untested technology / mechanism of action
The mRNA approach may be new from a product approval perspective. But mRNA has been researched in a number of areas outside viral vaccinology, such as cancer immunotherapies, cancer vaccines, and protein replacement.
Formulating and delivering mRNA successfully is no easy feat. And it has taken years to reach this point.
Whether the current imminent successes in the vaccine space will translate into success in other therapeutic areas and indications remains an open question. So is this “untested” technology? We are not prepared to go that far.
Two mRNA product are about to be approved, with more on the way. We think it is fair to say that mRNA is in fact tested, and will likely get even better.
More fundamentally, and judging by social media, there is a basic lack of understanding of what mRNA is, and how that actually results in a successful vaccine.
The lack of basic science education is a huge problem that really shows itself in times like these.
As an industry, we can do a better job of communicating what these technologies and products are.
But without an understanding of the basics, will those messages get lost or twisted into something negative? Judging by social media, they already are.
The vaccine is not needed
There is a subset of ideas that fall under this category.
- The survival rate is >99%, hence the vaccine is not needed.
It is certainly true that the case fatality rate is much lower than it was in the Spring. The current increases in hospitalizations and deaths are driven by increasing numbers of cases, and not a lack of expertise on how to manage these patients.
But the fatality rate is not zero. And like the influenzas, there are long-term sequelae associated with SARS-CoV-2 which are even worse.
So, a high survival rate is not a logical reason to proceed without a vaccine approach.
- COVID-19 is a disease of the aged who will soon succumb to this or something else anyway. So a vaccine for anyone over the age of x is not needed.
Ah, yes. The “old people don’t need it” argument.
It’s a horrible thought, to be sure. And one, frankly, which we will not acknowledge any further.
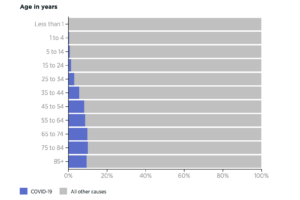
But if you look at the mortality data carefully, there are plenty of COVID-19 patients well below “old age.”
Patients in the 55-64 range are dying at roughly the same rate as those over the age of 85.
So unless you consider 55 years “old” (which we do not), then this argument falls apart a second time.
However, it does point to the issue of comorbidities which increases the probability of death due to COVID-19, like the metabolic diseases.
In a study published in April, comorbidities associated with positive COVID-19 infections were hypertension, obesity, and diabetes.
To say that comorbidities increase your chances of dying from COVID-19 should not be a surprise. Indeed, this is true for many other conditions, including influenza.
Complicating this is the observation that morbidity and mortality rises quickly as a function of age, especially over the age of 60.
While we all argue about the benefits (or lack thereof) of wearing masks and social distancing, we also find various local and national governments closing gymnasia and even discouraging outdoor recreation.
But what we should be encouraging is the opposite: fitness and healthy diets to reduce hypertension, reduce obesity and reduce diabetes.
In a sense, SARS-CoV-2 represents a great opportunity to convey the message that fitness is a cheap and easy way to prevent disease.
- Masks and social distancing are enough to keep deaths low. We need compliance!
The debate about whether or not masks work is lengthy and complex. So we will not delve into it here.
What is clear from our reading of the literature and various opinions is that masks are not a 100% guarantee of protection. They do protect to a certain degree, and under certain conditions.
But to see a rising number of cases and say that those cases will immediately start to fall once a mask mandate is initiated is a bit simplistic.
Thus, the uncertainty surrounding the effectiveness of mask mandates supports the need for rapid and widespread vaccination.
Implications
Social media can be a wonderful source of both education and entertainment. But can also be an absolute cesspool of misinformation and bizarre statements which can spread very quickly.
Pre-internet, nonsensical ideas came from people at work or at the local pub. Nowadays, they can come from anywhere via the little electronic doodad in our pockets.
We can avoid these conversations, of course. After all, we usually have better things to do.
But as representatives of our industry, we should think about ways to combat this misinformation. Especially if it can help drive vaccine compliance and safer socialization practices as we head into 2021.